


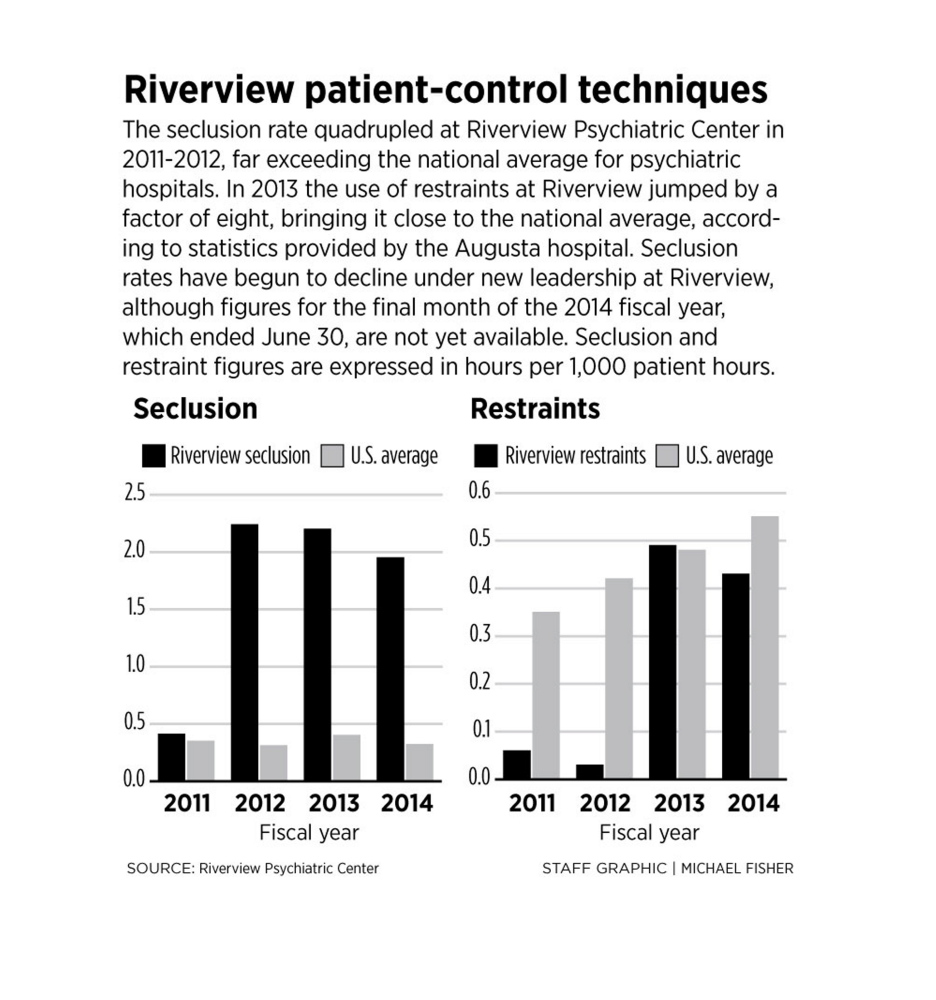
Riverview Psychiatric Center’s use of seclusion on its patients – a technique frowned upon by the mental health community for being a threat to patient health – jumped to more than seven times the national average in 2012, according to reports posted online by the hospital. The annual rate has remained high since, although there are signs of recent improvement.
The state-run hospital secludes agitated patients by forcing them into a padded isolation room, where they are checked on periodically by medical staff to determine if they are ready to be released. Federal and state reports have pointed to cases where Riverview has isolated patients for several hours at a time, and routinely sent some patients to the padded room for weeks. A report surfaced last month that revealed officers pepper-sprayed a defenseless, naked woman, then restrained and secluded her for hours despite the fact that she was complying with orders and not threatening staff.
Additional Images

Riverview employees failed to comply with the law by not reporting the December 2013 incident to state investigators for months, according to a state investigative report.
Riverview’s seclusion rates paint a picture of the psychiatric hospital as a continuing practitioner of discredited methods.
Seclusion should be extremely rare and used as a last resort, said Greg Smith, the former CEO of Allentown State Hospital in Pennsylvania and a national expert on reducing the use of the techniques. Nationally, seclusion and restraint rates have plummeted “dramatically” in recent decades, Smith said, although there are still examples of institutions that employ the techniques at a higher rate.
“In some cases, deaths have occurred,” said Smith, who has heard about Riverview’s problems but is hopeful that recent changes touted by Riverview’s acting Superintendent Jay Harper will prove fruitful. “(Riverview) is how not to do it, and it demonstrates what can go wrong. Nine and a half times out of 10, you can be successful in redirecting a patient into a therapeutic dialogue.”
Smith said seclusion and restraint are not treatment, can be harmful to a patient’s mental health, and hospitals that use the techniques liberally are not safer for employees.
While Riverview’s seclusion rate is high, the use of restraints more closely mirrors the national average, and was lower than the national average in 2011 and 2012.
Riverview is currently under intense scrutiny after losing $20 million in federal funding, partly because of patient abuse, and other issues that have led to substandard patient care.
FACILITY UNDER SCRUTINY
Former and current employees have come forward describing a dysfunctional and confrontational work culture at Riverview that allowed abuse to occur far too often, describing scenes where workers taunted, hit and tackled patients or withheld food.
The U.S. Centers for Medicare and Medicaid Services decertified Riverview in September 2013 after finding that corrections officers housed at Riverview used stun guns and handcuffs on patients. Other problems with patient care also surfaced, including a lack of treatment plans and training for employees.
In March, former Riverview Superintendent Mary Louise McEwen was fired, replaced shortly thereafter by Harper, a former Riverview patient advocate with the Disability Rights Center.
Harper did not respond to requests for comment, but he has previously outlined a number of reforms underway to limit the use of seclusion and restraint. Harper has also pointed to statistics that show, in recent months, that seclusion use has declined. The monthly reports show a sharp decline in seclusion rates from February through May, the latest month available.
But those numbers are in question and will be closely examined, according to a state agency charged with investigating Riverview. Beth Ashcroft, director of the Office of Program Evaluation and Government Accountability, said last month that her agency is examining the accuracy of the numbers; that the process used to collect data has inherent weaknesses; and that there is reason to doubt the integrity of the data. She did not go into further detail because the investigation is pending.
Harper has said he’s confident in the numbers, and that they will show that the hospital’s work culture has permanently changed to use seclusion or restraint only as a last resort.
Arlene Edson, the patient who was pepper-sprayed in December, said she has been in seclusion and restraints more than 10 times in the three years that she’s been at Riverview, including most recently a few weeks ago. In September, she said, she banged her head against a window because she was frustrated. The staff responded by strapping her to a bed and secluding her for about 90 minutes, Edson said.
“I don’t trust anybody here” after the pepper spray incident, she said.
A 2013 Centers for Medicare and Medicaid Services report gave examples of when seclusion was used inappropriately, including one patient who was in isolation for months and was allowed outside of the padded room for only five hours daily, and another patient who was in the seclusion room for several days in a row.
Tina Ashlock, a former Riverview nurse who resigned in January, said she saw the seclusion room being used too often, and in some cases patients were kept in there for weeks at a time.
MIX OF PATIENTS HAS CHANGED
For several years prior to 2012, seclusion use more closely matched the national average, according to the reports. But in 2012, the seclusion rate suddenly skyrocketed.
Why is not entirely clear, but Daniel Wathen, the court master charged with making sure that Riverview is treating patients well and complying with a court-ordered consent decree, has been monitoring the seclusion and restraint rates for years.
Wathen said he believes one factor is a change in the mix of patients at Riverview.
The Augusta hospital – unlike the state’s other mental institution, the Dorothea Dix Psychiatric Center in Bangor – is the only hospital that accepts forensic patients, who are sent there by the criminal court system.
While the 92-bed facility is split roughly evenly between forensic and civil patients, in 2011 or 2012 there was a surge in forensic patients, Wathen said. Some of the patients were more difficult to handle, and there was more mixing of forensic and civil patients, which also caused conflicts, Wathen said.
Additionally, in March 2013 state corrections officers and sheriff’s deputies were brought into Riverview after a patient hit and stabbed a pregnant employee with a pen.
Wathen said he believes the officers and the hospital staff never meshed.
“The corrections officers were not managed well by the clinical staff. They (officers) sort of became free agents,” said Wathen, explaining that the officers would be involved in dealing with patients in incidents that should have been handled entirely by the medical staff.
Despite complaints about the presence of corrections officers, they remained at Riverview until March, when they were replaced by security guards and Capitol Police.
Harper has said that the role of security guards and Capitol Police is being de-emphasized, and their contact with patients will be limited.
Judith Dorsey, a licensed social worker and former Riverview employee who began working there in 2009, said she did notice the use of seclusion more after she had been at the hospital for two years.
She said it’s difficult to know why it was used more, other than perhaps patients were coming to the hospital that were more difficult to deal with because they had abused bath salts. Dorsey left the hospital this summer and has been critical of its management.
Since 2012, Riverview’s patients have been held in seclusion for about two hours for every 1,000 patient hours at the hospital, far above the national average, which has stayed steady at about 30 minutes.
INSTITUTING REFORMS
Harper, the new superintendent, has touted a number of reforms that he says are already making a difference.
The changes include additional staff training to de-escalate agitated patients and hiring 16 “acuity specialists” whose job is specifically to defuse situations. Also, Harper has said, patients will not be restrained or secluded until a psychiatrist has observed them in person, which he says will be an incentive for staff to employ other methods of calming patients.
Every restraint and seclusion incident is now evaluated after the fact, Harper said, and the staff notes what could have been done differently to avoid the techniques.
Smith, the Pennsylvania expert on seclusion and restraint, said that staff buy-in and leadership being committed to change makes a big difference on whether reforms will succeed.
Smith said he would personally arrive at the scene at the Allentown hospital he managed when a situation was escalating.
“The CEO has to be personally involved in what’s going on,” Smith said. “That’s a deterrent for the staff to do or say something stupid.”
Smith said specific policy changes are also important, to make it clear under what conditions a patient can be secluded or restrained.
If leadership commits to the changes, and the staff is adequately trained, Smith said that the numbers can quickly and permanently turn around.
Helen Bailey, the attorney for the Disability Rights Center, said it will be difficult for Harper to change the work culture at Riverview – which opened in 2004 to replace the former Augusta Mental Health Institute – but so far the center is encouraged by Harper’s willingness to listen.
“We feel it’s moving in the right direction,” Bailey said.
Dorsey, the former Riverview social worker, said she is unimpressed by the changes so far, and that the dysfunctional work culture runs deep.
“These weak reassurances (by Harper) are not enough,” Dorsey said. “What are they actually doing to make it less antagonistic toward the clients?”
Send questions/comments to the editors.

Comments are no longer available on this story